
- Module 3
- Module 2
- Module 1
CBL No: 06 SENARIO: A 49-years old man with a history of congenital heart disease has a successful cardiac transplant 6 months ago. He is now admitted to the hospital in severe agitation. He is found to have a blood pressure of 170/110 mm hg, heart rate 130, respiration 35, sweating and cutaneous vasoconstriction. He admits to it self-injecting methamphetamine 4 hours previously. How does methamphetamine increase blood pressure? Normally, heart rate would be greatly reduced with this degree of drug-induced hypertension. Why is this patient’s heart rate elevated Learning outcomes: Mechanism of action of Methamphetamine. Adverse effect (short + long term).
Clinical use of methamphetamines.
Effect of dopamine, epinephrine and nor- epinephrine on heart.
CBL No: 05 SENARIO: Mrs Jameel, 45 years of age, is a housewife. Since last few months she was feeling fatigue of shoulder muscle while combing her hair. She had to perform some unusual physical work when her family was to move into a new residence and all the luggage and house hold was to be packed for shifting. She felt extremely weak during the activity and was compelled to take rest at short intervals. Learning outcomes: What is Myasthenia gravis? Explain etiology and patho-physiology of the disease.
Analyze the Approaches to pharmacotherapy of myasthenia gravis.
Enlist the classification of anticholinesterase drugs.
Explain the mechanism of action of anticholinesterases.
Discuss the adverse effects of anticholinesterases and their control
How to distinguish between cholinergic crisis and myasthenia crisis.
Discuss the uses of anticholinesterases.
Identify the drugs that may precipitate myasthenia gravis.
Learning resources: Basic and clinical Pharmacology by Bertram G Katzung 13th Edition The Pharmacological Basis of Therapeutics by Goodman & Gilman 12th Edition
Current Medical Diagnosis and treatment- 2015
CBL 04 A 68-year-old man presents with a complaint of lightheadedness on standing that is worse after meal and in hot environment. Symptoms started about 4 year ago and have slowly progressed to the point that he is disabled. He is fainted several times, but always recovers consciousness almost as soon as he falls. Review of symptoms reveals slight worsening of constipation, urinary retention out of proportion prostate size, and decrease sweating. He is otherwise healthy with no history of hypertension diabetes, orparkinson’s disease. Because of his urinary retention, he was placed on the α1 antagonist tamsulosin but he could not tolerate it because of worsening of orthostatic hypotension. Physical examination revealed a blood pressure of 167/84 mm Hg supine and 106/55 mm Hg standing. There was an inadequate compensatory increase in heart rate (from 84 to 88 bpm), considering the degree of orthostatic hypotension. Physical examination is otherwise unremarkable with no evidence of peripheral neuropathy or parkinsonian features. Lab examinations are negative expect for plasma norepinephrine, which is low at 98 pg/ml (normal is 250-400 pg/ml for his age). A diagnosis of pure autonomic failure is made, based on the clinical picture & the absence of drug that could induce orthostatic hypotension and disease commonly associated with autonomic neuropathy (e.g, diabetes, parkinso’s disease). What precaution should this patient observe in using sympathomimetic drugs? Can such drugs be used in his treatment? Learning outcomes: What are the physiological effect of catecholomines on body. Classification of sympathomimetic drugs.
Sites of action & effects on different system.
Adverse effects of sympathomimetic drugs.
Clinical uses of sympathomimetic drug.
CBL 03 A 16-year-old female come to ER, four hours after ingestion of insecticides (organophosphate). ON EXAMINATION 1. Altered consciousness, pupil constricted, Frothing from mouth 2. On auscultation; Tachypnoea and crepitation VITALS: Pulse 60/min, Respiratory 30/min, B.P 90/60 mmHg The intern on duty started I.V fluids and gave antidote pralidoxime but the condition of the patient further deteriorated, until physician came and started atropine I/v in small doses after fix intervals. The intern was curios & asked clinical pharmacologist about the role of antidote. He explained the role of antidote in this case by a graph.
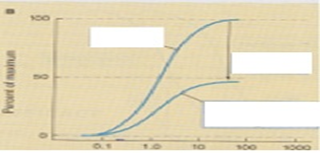
TASK: Interpret the graph and discuss the role of antagonist drugs and their types. Learning outcomes: Interpret the concept of agonist & antagonists
Explain the Types of antagonism
Understand the graph and ability to draw graph from given information.
Explain the mechanism of action of organophosphate.
Correlate the signs & symptoms of organophosphate poisoning
Explain the Role of atropine & oximes in treatment
CBL 02 A 17- year old, patient known case of asthma was prescribed the grad tablet (theophylline) by the physician 600mg/day in two divided doses. He took four tablets of 300mg in 24 hours and came in ER with complain of nausea, headache, G.I distress, tachycardia and his ECG indicated arrhythmia. He was anxious and asked his physician that he never developed toxic effect whenever he took analgesics in high doses. INVESTIGATION: Blood theophylline level………22mg/l Serum keratinize 1.2mg/dl Serum urea 18mg/dl Liver function test (L.F.T) were normal TASK Discus the development of toxic effect and related Pharmacologic parameters. Learning outcomes: Concept of safety & efficacy Therapeutic index Concept of toxicity Factors effecting dose and toxicity Concept of correlation of half-life e- dose adjustment CBL 01 SENARIO: A group of research student conducted a preclinical trial of two different drugs to establish safely and efficacy and to study Pharmacokinetic and Pharmacodynamic profile. Two different Rabbits of same size were taken and injected with either one of the drug labeled as A & B. They collected serial blood sample from each rabbit after fix intervals and measured drugs level and then plotted a graph to study the plasma concentration rate of elimination of drugs from the body.
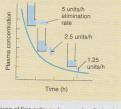
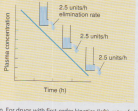
TASK Interpret the graph and discuss and compare the Pharmacokinetic profile of the drugs Learning outcomes: Explain the pharmacokinetics and pharmacodynamics Discuss the concept of half life and elimination of drug Explain the concept of zero order & first order kinetic. Interpret the concept of dose response curve Explain volume of distribution, clearance & bioavailability